摘 要: 目的 分析良、恶性甲状腺结节特征的临床差异。方法 采用细针穿刺细胞学和甲状腺彩色多普勒超声检查271例甲状腺结节患者(302个结节);其中,248个甲状腺结节有明确病理诊断,分析良、恶性甲状腺结节的临床差异。结果 248个甲状腺结节中,病理诊断良性结节195个,恶性结节53个。良性和恶性甲状腺结节的位置、回声、钙化性质、纵横比和边缘形态差异均有统计学差异(P<0.05)。多因素logistic回归分析显示,位于甲状腺中极和表现为低回声、微钙化、纵横比>1和边缘不光整是恶性甲状腺结节的独立危险因素(P<0.05)。结论 位于甲状腺中极、低回声、微钙化、纵横比>1和边缘不光整的甲状腺结节恶性的可能性较大。
关键词: 甲状腺结节;
Abstract: Objective To analyze the difference between benign and malignant thyroid nodules in clinical characteristics.Methods Fine needle aspiration cytology and thyroid ultrasound examination were performed in 271 patients with 302 thyroid nodules,of which 248 thyroid nodules had definite pathological diagnosis.The differences between benign and malignant thyroid nodules in clinical characteristics were analyzed.Results Of 248 thyroid nodules with pathological diagnosis,195 thyroid nodules were benign and 53 thyroid nodules were malignant.The differences in nodule location,echo,calcified property,aspect ratio and edge morphology were statistically different between benign and malignant thyroid nodules(P<0.05).Multivariate logistic regression analysis showed that the middle pole location,hypoechoic,microcalcification,aspect ratio >1 and uneven edges were the independent risk factors for malignant thyroid nodules(P<0.05).Conclusion The thyroid nodules located at the middle pole and with the manifestations of hypoechoic,microcalcification,aspect ratio >1 and uneven edges are more likely to be malignant.
Keyword: Thyroid nodule;
过去数十年间,甲状腺癌的高发病率得到了广泛的关注。有研究显示,20%~76%的普通人群中可以检出甲状腺结节,这一高检出率主要是由于临床上使用高分辨率超声进行常规检查[1,2]。研究已证实,超声下出现微钙化、实性低回声、边缘毛刺、纵横比>1等,提示甲状腺结节恶性风险明显增加[3]。在2018年美国临床内分泌医师学会年会上提出了甲状腺结节位于上极比下极恶性风险更高[4]。本研究旨在分析甲状腺结节良、恶性的影响因素。
资料与方法
一、一般资料
选取2016年5月—2019年5月就诊于我院内分泌科的甲状腺结节患者271例,共302个结节。所有患者接受了甲状腺彩色多普勒超声以及甲状腺结节细针穿刺细胞学(FNAC)检查。其中男73例,女198例,年龄20~68(40.63±11.74)岁。排除既往有甲状腺相关手术史的患者。
二、方法
1.超声检查
采用HI Vision Preirus型彩色多普勒超声诊断仪(日本HITACHI公司),探头频率7.5~13.0 MHz。由2名具有5年以上经验的超声科医师对271例患者的302个结节进行检查,意见不一致时经协商达成一致。超声具体特征包括结节位置、成分、边缘、钙化、形状、回声、大小。
2. FNAC检查
采用2人合作模式,1人操作超声仪器,1人进行细针穿刺操作。患者选取仰卧位,暴露颈前区,根据甲状腺结节位置选取最佳进针角度及路径;一次性细针无菌注射器在超声引导下穿进甲状腺结节,保证针尖位于结节内,适时提拉注射器,1个结节取材3次。
三、统计学处理
采用SPSS 22.0软件进行统计学分析。计数资料行χ2检验;影响因素采用多因素logistic回归分析;P<0.05为差异有统计学意义。
结 果
一、甲状腺结节良、恶性的单因素分析
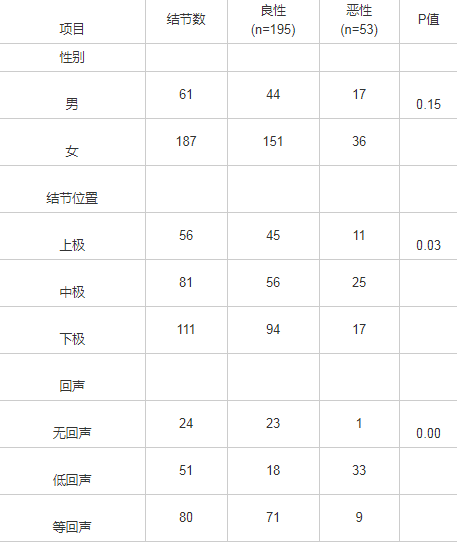
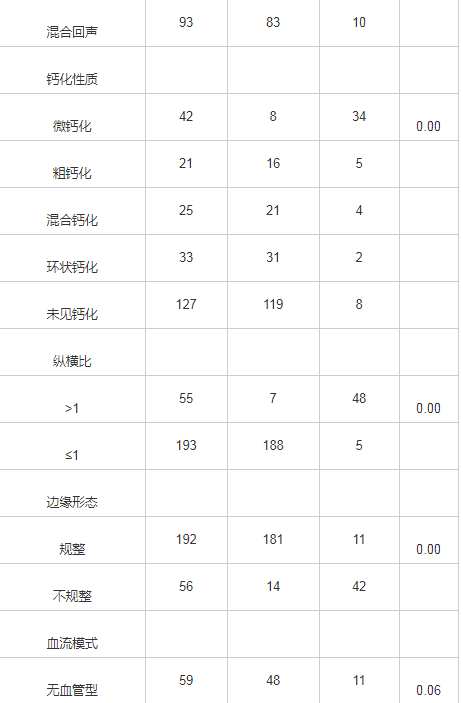
302个甲状腺结节接受了FNAC,由于穿刺细胞数量不够以及受结节性质、穿刺医生操作等影响会有5%~15%假阴性,最终248个甲状腺结节有明确的病理诊断,其中195个良性,53个恶性。单因素分析显示,良性和恶性甲状腺结节位置、回声、钙化性质、纵横比、边缘形态有统计学差异(P<0.05),性别、血流模式无统计学差异(P>0.05)(表1)。
表1 248个甲状腺结节良、恶性的单因素分析(个)
二、甲状腺结节良、恶性的多因素分析
以结节位置、回声、钙化性质、纵横比、边缘形态为自变量,以甲状腺结节良、恶性为因变量,进行多因素logistic回归分析,发现位于中极、低回声、微钙化、纵横比>1、边缘不光整是甲状腺结节恶性的独立危险因素(P<0.05)(表2)。
表2 多因素logistic回归分析

讨 论
近些年,甲状腺结节的发病率呈现逐年上升的趋势,而甲状腺癌的发生率在近10年来增加了2~3倍,且发病年龄趋于年轻化[5]。因此,如何有效建立一个临床综合评估系统对甲状腺结节进行风险评估,如何在早期鉴别甲状腺结节的良、恶性已成为临床诊治的重点和难点。
本研究显示,女性甲状腺结节的患病率高于男性,而女性甲状腺结节恶性率低于男性,但差异无统计学意义,这提示甲状腺良、恶性与性别无明显关系。目前彩色多普勒超声仍是临床上诊断甲状腺结节良、恶性的首选,病理检查则是诊断甲状腺良、恶性的金标准。良性和恶性甲状腺结节的结节位置、回声、钙化性质、纵横比、边缘形态有统计学差异,进一步行多因素logistic回归分析发现,低回声、微钙化、纵横比>1、边缘不光整是甲状腺结节恶性的独立危险因素,与相关研究结果一致[6,7]。有研究证实,结节内钙化是甲状腺癌发生的危险因素[8],与本研究结果一致。本研究中,甲状腺结节位于甲状腺下极的患病率较高,与相关研究结果一致[9,10],可能与滤泡旁细胞的聚集有关[11],尚需要后期研究进一步去验证。多因素logistic回归分析发现,位于中极是甲状腺结节恶性的独立危险因素,推测可能与发生淋巴结转移的甲状腺乳头状癌常常见于甲状腺上极或中极有一定关联[12,13]。本研究仍存在一定的局限性,FNAC诊断甲状腺结节可能会有假阴性出现,而且不同超声医生对结节的良、恶性评估不一致,会出现甲状腺结节穿刺的选择偏倚。
参考文献
[1] Durante C,Grani G,Lamartina L,et al.The diagnosis and management of thyroid nodules:a review[J].JAMA,2018,319(9):914-924.
[2] Sherwood G,Nickel B.Integrating quality and safety competencies to improve outcomes:application in infusion therapy practice[J].J Infus Nurs,2017,40(2):116-122.
[3] 聂芳,汪延芳,耿祥亮,等.不同标准TI-RADS分级对甲状腺癌的价值探讨[J].中国超声医学杂志,2016,32(11):967-970.
[4] Zhang F,Oluwo O,Castillo FB,et al.Thyroid nodule location on ultrasonography as a predictor of malignancy[J].Endocr Pract,2019,25(2):131-137.
[5] Dal Maso L,Lise M,Zambon P,et al.Incidence of thyroid cancer in Italy,1991-2005:time trends and age period-cohort effects[J].Ann Oncol,2011,22(4):957-963.
[6] Ahmed S,Johnson PT,Horton KM,et al.Prevalence of unsuspected thyroid nodules in adults on contrast enhanced 16- and 64-MDCT of the chest[J].World J Radiol,2012,4(7):311-317.
[7] Shetty SK,Maher MM,Hahn PF,et al.Significance of incidental thyroid lesions detected on CT:correlation among CT,sonography,and pathology[J].Am J Roentgenol,2006,187(5):1349-1356.
[8] 吴丹妮,胡蕴,毛晓明.甲状腺结节1476例临床分析[J].江苏医药,2018,44(12):1380-1383.
[9] Schmid KW.Histopathology of C cells and medullary thyroid carcinoma[J].Recent Results Cancer Res,2015,204:41-60.
[10] Tajiri K,Hirokawa M,Suzuki A,et al.Can ultrasound alone predict papillary thyroid carcinoma with desmoid-type fibromatosis?A retrospective analysis of 13 cases,focusing on the stromal area[J].Ultrasound Int Open,2018,4(2):E39-E44.
[11] Rocha TG,Rosario PW,Silva AL,et al.Ultrasonography classification of the american thyroid association for predicting malignancy in thyroid nodules >1 cm with indeterminate cytology:a prospective study[J].Horm Metab Res,2018,50(8):597-601.
[12] Xiang D,Xie L,Xu Y,et al.Papillary thyroid microcarcinomas located at the middle part of the middle third of the thyroid gland correlates with the presence of neck metastasis[J].Surgery,2015,157(3):526-533.
[13] Zeng RC,Li Q,Lin KL,et al.Predicting the factors of lateral lymph node metastasis in papillary microcarcinoma of the thyroid in eastern China[J].Clin Transl Oncol,2012,14(11):842-847.





