当地时间2月28日,由国家卫健委高级别专家组组长、中国工程院院士钟南山领衔的“中国2019新型冠状病毒疾病的临床特征”研究论文在顶级医学期刊《新英格兰医学杂志》(NEJM)上在线公开发表。该研究纳入了来自2019年12月11日至2020年1月29日来自全国31个省(市)共552家医院的1099例确诊新冠肺炎患者。中英文全文如下,文后附英文原文免费下载!
Clinical characteristics of 2019 novel coronavirus infection in China
2019年中国新型冠状病毒感染的临床特点
Abstract
摘 要
Background: Since December 2019, acute respiratory disease (ARD) due to 2019 novel coronavirus (2019-nCoV) emerged in Wuhan city and rapidly spread throughout China. We sought to delineate the clinical characteristics of these cases.
背景:自2019年12月以来,武汉市出现了由2019年新型冠状病毒(2019-nCoV)引起的急性呼吸系统疾病(ARD),并迅速在中国各地蔓延。我们试图描述这些病例的临床特征。
Methods: We extracted the data on 1,099 patients with laboratory-confirmed 2019-nCoV ARD from 552 hospitals in 31 provinces/provincial municipalities through January 29th, 2020.
方法:从31个省(市)的552家医院抽取到2020年1月29日的1099例实验室确诊病例资料。
Results: The median age was 47.0 years, and 41.90% were females. Only 1.18% of patients had a direct contact with wildlife, whereas 31.30% had been to Wuhan and 71.80% had contacted with people from Wuhan. Fever (87.9%) and cough (67.7%) were the most common symptoms. Diarrhea is uncommon. The median incubation period was 3.0 days (range, 0 to 24.0 days)。 On admission, ground-glass opacity was the typical radiological finding on chest computed tomography (50.00%)。 Significantly more severe cases were diagnosed by symptoms plus reverse-transcriptase polymerase-chain-reaction without abnormal radiological findings than non-severe cases (23.87% vs. 5.20%, P<0.001)。 Lymphopenia was observed in 82.1% of patients. 55 patients (5.00%) were admitted to intensive care unit and 15 (1.36%) succumbed. Severe pneumonia was independently associated with either the admission to intensive care unit, mechanical ventilation, or death in multivariate competing-risk model (sub-distribution hazards ratio, 9.80; 95% confidence interval, 4.06 to 23.67)。
结果:中位年龄47.0岁,女性41.90%.只有1.18%的患者直接接触过野生动物,31.30%的患者去过武汉,71.80%的患者接触过武汉人。发热(87.9%)和咳嗽(67.7%)是最常见的症状。腹泻是不常见的。中位潜伏期为3.0天(0-24.0天)。入院时,磨玻璃样阴影是胸部电脑断层摄影的典型影像学表现(50.00%)。症状加逆转录聚合酶链反应无异常影像学表现的危重病例明显多于非危重病例(23.87%对5.20%,P<0.001)。82.1%的患者出现淋巴细胞减少。55例(5.00%)进入重症监护病房,15例(1.36%)死亡。在多元竞争风险模型中,重症肺炎与重症监护病房入院、机械通气或死亡独立相关(亚分布危险比,9.80;95%可信区间,4.06至23.67)。
Conclusions: The 2019-nCoV epidemic spreads rapidly by human-to-human transmission. Normal radiologic findings are present among some patients with 2019-nCoV infection. The disease severity (including oxygen saturation, respiratory rate, blood leukocyte/lymphocyte count and chest X-ray/CT manifestations) predict poor clinical outcomes.
结论:2019年nCoV疫情通过人传人传播迅速。部分2019例nCoV感染患者的影像学表现正常。疾病的严重程度(包括血氧饱和度、呼吸频率、白细胞/淋巴细胞计数和胸部X线/CT表现)预示着不良的临床结果。
Key words: 2019 novel coronavirus; acute respiratory disease; transmission; mortality; risk factor
关键词:2019年新冠状病毒;急性呼吸道疾病;传染;死亡率;风险因素
Abstract: 249 words; main text: 2677 words
摘要:249字;正文:2677字
Funding: Supported by Ministry of Science and Technology, National Health Commission, National Natural Science Foundation, Department of Science and Technology of Guangdong Province.
经费来源:科技部、国家卫生委员会、国家自然科学基金、广东省科技厅。
Conflict of interest: None declared.
利益冲突:未声明。
Running head: 2019-nCoV in China
运行负责人:2019中国nCoV

配图:钟南山研究团队
1. Introduction
1、引言
In early December 2019, the first pneumonia cases of unknown origins were identified in Wuhan city, Hubei province, China [1]. High-throughput sequencing has revealed a novel betacoronavirus that is currently named 2019 novel coronavirus (2019-nCoV) [2], which resembled severe acute respiratory syndrome coronavirus (SARS-CoV) [3]. The 2019-nCoV is the seventh member of enveloped RNA coronavirus (subgenus sarbecovirus, Orthocoronavirinae subfamily) [3]. Evidence pointing to the person-to-person transmission in hospital and family settings has been accumulating [4-8].
2019年12月初,中国湖北省武汉市首次发现不明原因肺炎病例。高通量测序发现一种新型冠状病毒,目前命名为2019年新型冠状病毒(2019- ncov)[2],与严重急性呼吸综合征冠状病毒(SARS-CoV)[3]相似。2019-nCoV是包膜RNA冠状病毒(sarbecvirus亚属,Orthocoronavirinae亚科)[3]的第七成员。越来越多的证据表明,在医院和家庭环境中存在人际传播[4-8].
The World Health Organization has recently declared the 2019-nCoV a public health emergency of international concern [9]. As of February 5th, 2020, 24,554 laboratory-confirmed cases have been documented globally (i.e., the USA, Vietnam, Germany) [5,6,9,10]. 28,018 laboratory-confirmed cases and 563 death cases in China as of February 6th, 2020 [11]. Despite the rapid spread worldwide, the clinical characteristics of 2019-nCoV acute respiratory disease (ARD) remain largely unclear. In two recent studies documenting the clinical manifestations of 41 and 99 patients respectively with laboratory-confirmed 2019-nCoV ARD who were admitted to Wuhan, the severity of some cases with 2019-nCoV ARD mimicked that of SARS-CoV [1,12]. Given the rapid spread of 2019-nCoV, an updated analysis with significantly larger sample sizes by incorporating cases throughout China is urgently warranted. This will not only identify the defining epidemiological and clinical characteristics with greater precision, but also unravel the risk factors associated with mortality. Here, by collecting the data from 1,099 laboratory-confirmed cases, we sought to provide an up-to-date delineation of the epidemiological and clinical characteristics of patients with 2019-nCoV ARD throughout mainland China.
世界卫生组织最近宣布2019-nCoV为国际关注的突发公共卫生事件。截至2020年2月5日,全球共有24,554例实验室确诊病例(即,美国,越南,德国)[5,6,9,10].截至2020年2月6日,中国实验室确诊病例28018例,死亡病例563例。尽管在全球范围内迅速传播,但2019-nCoV急性呼吸道疾病(ARD)的临床特征仍不清楚。最近的两项研究分别记录了实验室确诊的2019-nCoV ARD的41例和99例的临床表现,其中部分2019-nCoV ARD的严重程度与SARS-CoV相似[1,12].鉴于2019-nCoV的迅速传播,迫切需要通过纳入中国各地的病例更新分析,使样本量大大增加。这不仅将更精确地确定确定的流行病学和临床特征,而且还将揭示与死亡率相关的危险因素。在此,通过收集1099例实验室确诊病例的数据,我们试图为中国大陆2019-nCoV ARD患者的流行病学和临床特征提供最新的描述。
2. Methods Data sources
2、研究方法与数据来源
We performed a retrospective study on the clinical characteristics of laboratory-confirmed cases with 2019-nCoV ARD. The initial cases were diagnosed as having 'pneumonia of unknown etiology', based on the clinical manifestations and chest radiology after exclusion of the common bacteria or viruses associated with community-acquired pneumonia. Suspected cases were identified as having fever or respiratory symptoms, and a history of exposure to wildlife in Wuhan seafood market, a travel history or contact with people from Wuhan within 2 weeks [13]. Cases were diagnosed based on the WHO interim guidance [14]. A confirmed case with 2019-nCoV ARD was defined as a positive result to high-throughput sequencing or real-time reverse-transcriptase polymerase-chain-reaction (RT-PCR) assay for nasal and pharyngeal swab specimens [1]. Only the laboratory-confirmed cases were included the analysis. The incubation period was defined as the duration from the contact of the transmission source to the onset of symptoms. The study was approved by the National Health Commission and the institutional board of each participating site. Written informed consent was waived in light of the urgent need to collect clinical data.
我们对2019-nCoV ARD实验室确诊病例的临床特征进行了回顾性研究。在排除与社区获得性肺炎相关的常见细菌或病毒后,根据临床表现和胸片学,最初的病例被诊断为“病因不明的肺炎”.疑似病例经确认有发热或呼吸道症状,有在武汉海鲜市场接触野生动物的历史,有2周内与来自武汉的人接触或旅行史。病例是根据世卫组织临时指南[14]诊断的。经鼻咽拭子标本[1]高通量测序或实时逆转录酶聚合酶链反应(RT-PCR)检测,确诊病例为2019-nCoV ARD阳性。只有实验室确诊病例纳入分析。潜伏期定义为从接触传播源到出现症状的时间。这项研究得到了国家卫生委员会和每个参与站点的机构委员会的批准。鉴于迫切需要收集临床数据,放弃了书面知情同意。
The epidemiological characteristics (including recent exposure history), clinical symptoms and signs and laboratory findings were extracted from electronic medical records. Radiologic assessments included chest X-ray or computed tomography. Laboratory assessments consisted of complete blood count, blood chemistry, coagulation test, liver and renal function, electrolytes, C-reactive protein, procalcitonin, lactate dehydrogenase and creatine kinase. The severity of 2019-nCoV ARD was defined based on the international guidelines for community-acquired pneumonia [15].
从电子病历中提取流行病学特征(包括近期接触史)、临床症状和体征以及实验室检查结果。放射学评估包括胸部x光或计算机断层扫描。实验室评估包括全血计数、血液化学、凝血试验、肝肾功能、电解质、c反应蛋白、降钙素原、乳酸脱氢酶和肌酸激酶。2019-nCoV ARD的严重程度是根据国际社区获得性肺炎[15]指南确定的。
The primary composite endpoint was the admission to intensive care unit (ICU), or mechanical ventilation, or death. Secondary endpoints comprised mortality rate, the time from symptom onset to the composite endpoint and each of its component. Because clinical observations were still ongoing, fixed time frame (i.e. within 28 days) was not applied to these endpoints.
主要的复合终点是重症监护病房(ICU),或机械通气,或死亡。次要终点包括死亡率、从症状出现到复合终点的时间及其各组成部分。由于临床观察仍在进行中,所以没有对这些终点应用固定的时间范围(即28天内)。
All medical records were copied and sent to the data processing center in Guangzhou, under the coordination of the National Health Commission. A team of experienced respiratory clinicians reviewed and abstracted the data. Data were entered into a computerized database and cross-checked. If the core data were missing, requests of clarification were immediately sent to the coordinators who subsequently contacted the attending clinicians. The definition of exposure to wildlife, acute respiratory distress syndrome (ARDS), pneumonia, acute kidney failure, acute heart failure and rhabdomyolysis are provided in the Supplementary Appendix.
在国家卫生健康委员会的协调下,所有的医疗记录被复制并发送到广州的数据处理中心。一组有经验的呼吸临床医师回顾并提取数据。数据被输入计算机化的数据库并反复核对。如果核心数据丢失,立即向协调员提出澄清要求,协调员随后联系主治医师。野生动物暴露、急性呼吸窘迫综合征(acute respiratory distress syndrome, ARDS)、肺炎、急性肾衰竭、急性心力衰竭和横纹肌溶解的定义见附录。
3. Laboratory confirmation
3、实验室确认
Laboratory confirmation of the 2019-nCoV was achieved through the concerted efforts of the Chinese Center for Disease Prevention and Control (CDC), the Chinese Academy of Medical Science, Academy of Military Medical Sciences, and Wuhan Institute of Virology. The RT-PCR assay was conducted in accordance with the protocol established by the World Health Organization [16]. Further details are available in the Supplementary Appendix.
通过中国疾病预防控制中心、中国医学科学院、军事医学科学院和武汉病毒学研究所的共同努力,2019-nCoV的实验室确认工作已经完成。RT-PCR检测按照世界卫生组织[16]制定的方案进行。更多详情见补充附录。
4. Statistical analysis
4、统计分析
Continuous variables were expressed as the means and standard deviations or medians and interquartile ranges (IQR) as appropriate. Categorical variables were summarized as the counts and percentages in each category. We grouped patients into severe and non-severe 2019-nCoV ARDaccording to the American Thoracic Society guideline on admission [15]. Wilcoxon rank-sum tests were applied to continuous variables, chi-square tests and Fisher's exact tests were used for categorical variables as appropriate. The risk of composite endpoints among hospitalized cases and the potential risk factors were analyzed using Fine-Gray competing-risk models in which recovery is a competing risk. The proportional hazard Cox model was used in sensitivity analyses. The candidate risk factors included an exposure history, greater age, abnormal radiologic and laboratory findings, and the development of complications. We fitted univariate models with a single candidate variable once at a time. The statistically significant risk factors, sex, and smoking status were included into the final models. The sub-distribution hazards ratio (SDHR) along with the 95% confidence interval (95%CI) were reported. All analyses were conducted with R software version 3.6.2 (R Foundation for Statistical Computing)。 Distribution map was plotted using ArcGis version 10.2.2.
连续变量以均值和标准差或中位数和四分位数范围(IQR)表示。分类变量被总结为每个类别中的计数和百分比。根据美国胸科协会关于入院[15]的指南,我们将患者分为严重和非严重2019-nCoV ARD.连续变量采用Wilcoxon秩和检验,分类变量适当采用卡方检验和Fisher精确检验。采用细灰色竞争风险模型分析住院患者的复合终点风险和潜在风险因素,其中康复是竞争风险。灵敏度分析采用比例危险系数Cox模型。可能的危险因素包括接触史、年龄、异常的放射学和实验室检查结果,以及并发症的发展。我们一次用一个候选变量拟合单变量模型。统计上显着的危险因素、性别和吸烟状况被纳入最终的模型。报告了子分布危险率(SDHR)和95%置信区间(95% ci)。所有分析均使用R软件版本3.6.2 (R统计计算基础)进行。使用ArcGis version 10.2.2绘制分布图。
5. Results
5、结果
Demographic and clinical characteristics
人口统计学和临床特征
Of all 1,324 patients recruited as of January 29th, 222 (16.8%) had a suspected diagnosis and were therefore excluded. The core data sets (including clinical outcomes and symptoms) of 3 patients were lacking due to the incompleteness of original reports, hence this report delineates 1,099 patients with 2019-nCoV ARD from 552 hospitals in 31 provinces/province-level municipalities (Fig. 1)。
截至1月29日,1324名患者中,222名(16.8%)有疑似诊断,因此被排除在外。由于原始报告的不完整性,3名患者的核心数据集(包括临床结果和症状)缺乏,因此本报告描述了31个省/直辖市552家医院1099名2019年NCO患者(图1)。
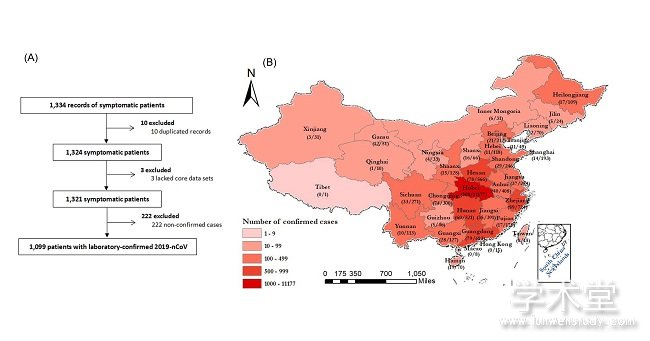
图1
The demographic and clinical characteristics are shown in Table 1. 2.09% were healthcare workers. A history of contact with wildlife, recent travel to Wuhan, and contact with people from Wuhan was documented in 1.18%, 31.30% and 71.80% of patients, respectively. 483 (43.95%) patients were local residents of Wuhan. 26.0% of patients outside of Wuhan did not have a recent travel to Wuhan or contact with people from Wuhan. The median incubation period was 3.0 days (range, 0 to 24.0)。
人口统计学和临床特征见表1.2.09%是医疗工作者。1.18%的患者有接触野生动物史,31.30%有近期到过武汉,71.80%有接触过武汉人。483例(43.95%)患者为武汉本地居民,26.0%的武汉以外地区患者近期未到武汉旅游或与武汉人接触。潜伏期中位数为3.0天(范围为0至24.0)。
The median age was 47.0 years (IQR, 35.0 to 58.0), and 41.9% were females. 2019-nCoV ARD was diagnosed throughout the whole spectrum of age. 0.9% of patients were aged below 15 years. Fever (87.9%) and cough (67.7%) were the most common symptoms, whereas diarrhea (3.7%) and vomiting (5.0%) were rare. 25.2% of patients had at least one underlying disorder (i.e., hypertension, chronic obstructive pulmonary disease)。 On admission, 926 and 173 patients were categorized into non-severe and severe subgroups, respectively. The age differed significantly between the two groups (mean difference, 7.0, 95%CI, 4.4 to 9.6)。 Moreover, any underlying disorder was significantly more common in severe cases as compared with non-severe cases (38.2% vs. 22.5%, P<0.001)。 There were, however, no marked differences in the exposure history between the two groups (all P>0.05)。
中位年龄47.0岁(IQR, 35.0 ~ 58.0岁),女性41.9%.2019-nCoV ARD的诊断跨越整个年龄谱。0.9%的患者年龄在15岁以下。发烧(87.9%)和咳嗽(67.7%)是最常见的症状,而腹泻(3.7%)和呕吐(5.0%)罕见。25.2%的患者至少有一种潜在的疾病(即、高血压、慢性阻塞性肺病)。入院时分别将926例和173例患者分为非严重组和严重组。两组间年龄差异有统计学意义(均值分别为7.0、95%CI、4.4 ~ 9.6)。此外,与非严重病例相比,严重病例(38.2%比22.5%,P<0.001)更常见。两组患者的暴露史无明显差异(P>0.05)。
Radiologic and laboratory findings at presentation
表现时的放射学和实验室检查结果
Table 2 shows the radiologic and laboratory findings on admission. Of 840 patients who underwent chest computed tomography on admission, 76.4% manifested as pneumonia. The most common patterns on chest computed tomography were ground-glass opacity (50.0%) and bilateral patchy shadowing (46.0%)。 Figure E1 in the Supplementary Appendix demonstrates the representative radiologic findings of two patients with non-severe 2019-nCoV ARD and another two patients with severe 2019-nCoV ARD. Despite these predominant manifestations, 221 out of 926 (23.87%) in severe cases compared with 9 out of 173 non-severe cases (5.20%) who had no abnormal radiological findings were diagnosed by symptoms plus RT-PCR positive findings (P<0.001)。 Severe cases yielded more prominent radiologic abnormalities on chest X-ray and computed tomography than non-severe cases (all P<0.05)。
表2显示入院时的放射学和实验室检查结果。840名病人在入院时接受了胸部计算机断层扫描,其中76.4%表现为肺炎。胸部计算机断层最常见的模式是毛玻璃阴影(50.0%)和双侧斑片状阴影(46.0%)。附录中的图E1显示了2例非严重2019-nCoV ARD患者和2例严重2019-nCoV ARD患者的典型影像学表现。尽管有这些主要表现,926例(23.87%)重症患者中有221例(23.87%),而在173例无放射学异常表现的非重症患者中有9例(5.20%)通过症状和RT-PCR阳性结果确诊(P<0.001)。严重病例在胸部x线及电脑断层摄影上的影像异常较非严重病例更为明显(P<0.05)
On admission, 82.1% and 36.2% of patients had lymphopenia and thrombocytopenia, respectively. Overall, leukopenia was observed in 33.7% of patients. Most patients demonstrated elevated levels of C-reactive protein, but elevated levels of alanine aminotransferase, aspartate aminotransferase, creatine kinase and D-dimer were less common. Severe cases had more prominent laboratory abnormalities (i.e., leukopenia, lymphopenia, thrombocytopenia, elevated C-reactive protein levels) as compared with non-severe cases (all P<0.05)。
入院时,82.1%的患者淋巴细胞减少,36.2%的患者血小板减少。总的来说,33.7%的患者出现白细胞减少。大多数患者c反应蛋白水平升高,但丙氨酸氨基转移酶、天冬氨酸氨基转移酶、肌酸激酶和d -二聚体水平升高较少见。严重的病例有更明显的实验室异常(即、白细胞减少、淋巴细胞减少、血小板减少、c反应蛋白水平升高(P均<0.05)。
Treatment and complications
治疗和并发症
Overall, oxygen therapy, mechanical ventilation, intravenous antibiotics and oseltamivir therapy were initiated in 38.0%, 6.1%, 57.5% and 35.8% of patients, respectively. All these therapies were initiated in significantly higher percentages of severe cases (all P<0.05)。 Significantly more severe cases received mechanical ventilation (non-invasive: 32.37% vs. 0%, P<0.001; invasive: 13.87% vs. 0%, P<0.001) as compared with non-severe cases. Systemic corticosteroid was given to 18.6% of cases and more so in the severe group than the non-severe patients (44.5% vs 13.7%, p<0.001)。 Moreover, extracorporeal membrane oxygenation was adopted in 5 severe cases but none in non-severe cases (P<0.001)。
总体而言,分别有38.0%、6.1%、57.5%和35.8%的患者开始接受氧疗、机械通气、静脉注射抗生素和奥司他韦治疗。所有这些治疗方法在严重病例中均有显着提高(P<0.05)。机械通气(无创:32.37% vs. 0%, P<0.001;侵袭性:13.87% vs. 0%, P<0.001)。18.6%的患者使用了全身性皮质类固醇,重症组比非重症组更多(44.5% vs 13.7%, p<0.001)。5例重症患者采用体外膜氧合,非重症患者未采用体外膜氧合(P<0.001)。
During hospital admission, the most common complication was pneumonia (79.1%), followed by ARDS (3.37%) and shock (1.00%)。 Severe cases yielded significantly higher rates of any complication as compared with non-severe cases (94.8% vs. 72.2%, P<0.001) (Table 3)。
住院期间最常见的并发症是肺炎(79.1%),其次是ARDS(3.37%)和休克(1.00%)。严重病例的并发症发生率明显高于非严重病例(94.8%比72.2%,P<0.001)(表3)。
Clinical outcomes
临床结果
The percentages of patients being admitted to the ICU, requiring invasive ventilation and death were 5.00%, 2.18% and 1.36%, respectively. This corresponded to 67 (6.10%) of patients having reached to the composite endpoint (Table 3)。
需要有创通气和死亡的ICU患者分别为5.00%、2.18%和1.36%.这相当于67例(6.10%)患者达到复合终点(表3)。
Results of the univariate competing risk model are shown in Table E1 in Supplementary Appendix. Severe pneumonia cases (SDHR, 9.803; 95%CI, 4.06 to 23.67), leukocyte count greater than 4,000/mm3 (SDHR, 4.01; 95%CI, 1.53 to 10.55) and interstitial abnormality on chest X-ray (SDHR, 4.31; 95%CI, 1.73 to 10.75) were associated with the composite endpoint (Fig. 2, see Table E2 in Supplementary Appendix)。 Sensitivity analyses are shown in Figure E2 in Supplementary Appendix.
单变量竞争风险模型的结果见附录表E1.重症肺炎病例(SDHR, 9.803;白细胞计数大于4000 /mm3 (SDHR, 4.01;胸部x线显示95%CI, 1.53 ~ 10.55)及间质异常(SDHR, 4.31;95%CI, 1.73 ~ 10.75)与复合终点相关(图2,见附录表E2)。灵敏度分析见附录图E2.
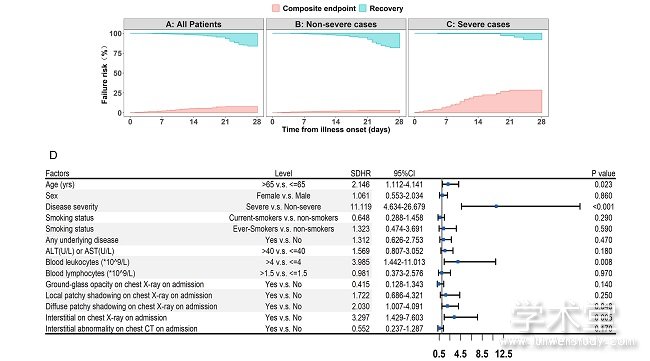
图2
6. Discussion
6、讨论
This study has shown that fever occurred in only 43.8% of patients with 2019-nCoV ARD on presentation but developed in 87.9% following hospitalization. Severe pneumonia occurred in 15.7% of cases. No radiologic abnormality was noted on initial presentation in 23.9% and 5.2% of severe and non-severe cases respectively while diarrhea was uncommon. The median incubation period of 2019-nCoV ARD was 3.0 days and it had a relatively lower fatality rate than SARS-CoV and MERS-CoV. Disease severity independently predicted the composite endpoint.
本研究表明,2019-nCoV ARD患者中仅有43.8%出现发热症状,但住院后出现发热症状的占87.9%.重症肺炎占15.7%.严重和非严重的病例中分别有23.9%和5.2%在最初的表现没有发现放射学异常,而腹泻则不常见。2019-nCoV ARD的中位潜伏期为3.0天,相对于SARS-CoV和MERS-CoV的致死率较低。疾病严重程度独立预测复合终点。
Our study provided further evidence of human-to-human transmission. Around only 1% of patients had a direct contact with wildlife, while more than three quarters were local residents of Wuhan, or had contacted with people from Wuhan. Most cases were recruited after January 1st, 2020.These findings echoed the latest reports, including the outbreak of a family cluster [4], transmission from an asymptomatic individual [6] and the three-phase outbreak patterns [8]. Our study cannot preclude the presence of 'super-spreaders'. The median incubation period was shorter than a recent report of 425 patients (3.0 days vs. 5.2 days) [8]. Our findings have provided evidence from a much larger sample size to guide the duration of quarantine for close contacts.
我们的研究为人际传播提供了进一步的证据。大约只有1%的患者与野生动物有过直接接触,而超过四分之三的患者是武汉当地居民,或与来自武汉的人有过接触。大多数病例是在2020年1月1日以后招募的。这些发现与最近的报告相呼应,包括一个家庭群集[4]的暴发、一个无症状个体[6]的传播以及[8]的三阶段暴发模式。我们的研究不能排除“超级传播者”的存在。中位潜伏期较近期报告的425例患者(3.0天vs. 5.2天)短。我们的发现为指导密切接触者的隔离期提供了来自更大样本量的证据。
Importantly, the routes of transmission might have contributed considerably to the rapid spread of 2019-nCoV. Conventional routes of transmission of SARS-CoV, MERS-CoV and highly pathogenic influenza consisted of the respiratory droplets and direct contact [17-19]. According to our latest pilot experiment, 4 out of 62 stool specimens (6.5%) tested positive to 2019-nCoV, and another four patients in a separate cohort who tested positive to rectal swabs had the 2019-nCoV being detected in the gastrointestinal tract, saliva or urine (see Tables E3-E4 in Supplementary Appendix)。 In a case with severe peptic ulcer after symptom onset, 2019-nCoV was directly detected in the esophageal erosion and bleeding site (Hong Shan and Jin-cun Zhao, personal communication)。 Collectively, fomite transmission might have played a role in the rapid transmission of 2019-nCoV, and hence hygiene protection should take into account the transmission via gastrointestinal secretions. These findings will, by integrating systemic protection measures, curb the rapid spread worldwide.
重要的是,传播途径可能对2019-nCoV的迅速传播有相当大的贡献。SARS-CoV、MERS-CoV和高致病性流感的常规传播途径包括飞沫和直接接触[17-19].根据我们最新的预试验,4 62份粪便标本2019 - ncov(6.5%)阳性,在一个单独的队列和另外四个病人阳性2019 - ncov直肠拭子已经被发现在胃肠道,唾液或尿液在补充附录E3-E4(见表)。出现症状后出现严重消化性溃疡的病例,直接在食管糜烂出血部位检测到2019-nCoV (Hong Shan and Jin-cun Zhao, personal communication)。综上所述,2019-nCoV的快速传播可能与污染物传播有关,因此,卫生防护应考虑通过胃肠道分泌物的传播。这些发现将通过综合系统的保护措施,遏制全球范围内的迅速蔓延。
We have adopted the term 2019-nCoV ARD which has incorporated the laboratory-confirmed symptomatic cases without apparent radiologic manifestations. Pneumonia was not mandatory for inclusion. 20.9% patients have isolated 2019-nCoV infection before or without the development of viral pneumonia. Our findings advocate shifting the focus to identifying and managing patients at an earlier stage, before disease progression.
我们采用了2019-nCoV ARD这一术语,它包含了实验室确诊的无明显放射学表现的症状病例。肺炎并不是强制纳入的。20.9%的患者在发生病毒性肺炎之前或未发生病毒性肺炎之前已分离出2019-nCoV感染。我们的发现主张将重点转移到在疾病进展之前的早期阶段识别和管理患者。
In concert of recent publications [1,8,12], the clinical characteristics of 2019-nCoV ARD mimicked those of SARS-CoV. Fever and cough were the dominant symptoms whereas gastrointestinal symptoms were rare, suggesting the difference in viral tropism as compared with SARS-CoV, MERS-CoV and influenza [20-22]. Notably, fever occurred in only 43.8% of patients on initial presentation and developed in 87.9% following hospitalization. Absence of fever in 2019-nCoV ARD is more frequent than in SARS-CoV (1%) and MERS-CoV infection (2%) [19] and such patients may be missed if the surveillance case definition focused heavily on fever detection [14]. Consistent with two recent reports [1,12], lymphopenia was common and, in some cases, severe. However, based on a larger sample size and cases recruited throughout China, we found a markedly lower case fatality rate (1.4%) as compared with that reportedly recently [1,12]. The fatality rate was lower (0.88%) when incorporating additional pilot data from Guangdong province (N=603) where effective prevention has been undertaken (unpublished data)。 Our findings were consistent with the national official statistics, reporting the mortality of 2.01% in China out of 28,018 cases as of February 6th, 2020 [11,23]. Early isolation, early diagnosis and early management might have collectively contributed to the marked reduction in mortality in Guangdong. Furthermore, dilution of health workforce as a result of central management (i.e., Wuhan JinYinTan Hospital) might have led to increased mortality rate. These findings will inform the mass public, clinicians and policy makers the true transmissability of 2019-nCoV which has resulted in a major social panic.
在近期发表的文献[1,8,12]中,2019-nCoV ARD的临床特征与SARS-CoV相似。发热、咳嗽为主要症状,胃肠道症状少见,提示与SARS-CoV、MERS-CoV、流行性感冒相比,病毒向性有差异[20-22].值得注意的是,最初出现发热症状的患者仅占43.8%,住院后出现发热症状的患者占87.9%.2019-nCoV ARD的无发热情况比SARS-CoV(1%)和MERS-CoV感染(2%)[19]更为常见,如果监测病例定义主要集中于发热检测[14],则此类患者可能会被遗漏。与最近的两篇报道一致[1,12],淋巴细胞减少是常见的,在某些情况下是严重的。然而,基于更大的样本量和中国各地招募的病例,我们发现与最近报道的相比,病死率显着降低(1.4%)[1,12].纳入广东省的其他试点数据(N=603)时,死亡率较低(0.88%),广东省采取了有效的预防措施(未发表的数据)。我们的研究结果与国家官方统计数据一致,截至2020年2月6日,中国28018例患者的死亡率为2.01%[11,23].早期隔离、早期诊断和早期治疗可能共同有助于广东死亡率的显着降低。此外,由于中央管理(即可能导致了死亡率的上升。这些发现将告知大众、临床医生和政策制定者2019-nCoV的真实传播能力,该病毒已经导致了一场重大的社会恐慌。
Our study has stratified patients with 2019-nCoV ARD based on the severity on admission according to international guidelines [15]. Severe cases had significantly higher risk of reaching the composite endpoint. The risk factors indicated the importance of taking into account the disease severity, laboratory findings, chest imaging findings in practice. The applicability of MuLBSTA score, an early warning model for predicting mortality in viral pneumonia, warrants further validation [25].
根据国际指南[15],我们的研究根据入院时的严重程度对2019-nCoV ARD患者进行了分层。严重病例达到复合终点的风险明显更高。危险因素表明,在实际工作中应考虑疾病的严重程度、实验室检查结果、胸部影像学检查结果。MuLBSTA评分是预测病毒性肺炎死亡率的早期预警模型,其适用性值得进一步验证。
Despite the markedly high phylogenetic homogeneity as compared with SARS-CoV, there are some clinical characteristics that differentiated 2019-nCoV from SARS-CoV, MERS-CoV, and seasonal influenza which have been more common in respiratory out-patient clinics and wards. Table E5 in Supplementary Appendix highlights the defining characteristics of these viruses, enabling clinicians to differentiate these diagnoses.
尽管与SARS-CoV相比具有明显高的系统发育同质性,但仍有一些临床特征可将2019-nCoV与SARS-CoV、MERS-CoV和季节性流感区分开来,这类流感在呼吸门诊诊所和病房中更为常见。附录中的表E5强调了这些病毒的定义特征,使临床医生能够区分这些诊断。
Our study has some notable limitations. First, some cases had incomplete documentation of the exposure history, symptoms and laboratory testing given the variation in the structure of electronic database among different participating site and the urgent timeline for data extraction. Some cases were diagnosed in out-patient settings where medical information was briefly documented and incomplete laboratory testing was applied. There was a shortage of infrastructure and training of medical staff in non-specialty hospitals, which has been aggravated by the burn-out of local medical staff in milieu of a surge of cases. Second, because many patients still remained in the hospital, we did not compare the 28-day rate of the composite endpoint. To mitigate the potential bias, we have applied the competing-risk model for analysis. Third, we might have missed asymptomatic or mild cases managed at home, and hence our cohort might represent the more severe end of 2019-nCoV ARD. However, there were a minority of patients who had no apparent radiologic manifestations, suggesting that we had included patients at the early stage of disease. Last, we took reference on the existing international guideline to define the severity of 2019-nCoV because of its global recognition [15].
我们的研究有一些明显的局限性。首先,考虑到不同参与地点电子数据库结构的差异和数据提取的紧急时间安排,一些病例的暴露史、症状和实验室检测记录不完整。一些病例是在门诊诊断的,那里的医疗信息被简要地记录下来,并且应用了不完整的实验室检测。非专科医院缺乏基础设施和医务人员培训,而在病例激增的情况下,当地医务人员疲惫不堪,使情况更加严重。其次,由于许多患者仍在住院,我们没有比较复合终点的28天生存率。为了减少潜在的偏差,我们采用了竞争风险模型进行分析。第三,我们可能错过了在家治疗的无症状或轻度病例,因此我们的研究对象可能代表2019-nCoV ARD的更严重结局。然而,有少数患者没有明显的放射学表现,这表明我们包括了早期的患者。最后,我们参考了现有的国际准则来定义2019-nCoV的严重性,因为它的全球认可度为[15].
In summary, 2019-nCoV elicits a rapid spread of outbreak with human-to-human transmission, with a median incubation period of 3 days and a relatively low fatality rate. Absence of fever and radiologic abnormality occurs in a substantial proportion of patients on initial presentation while diarrhea is uncommon. The disease severity is an independent predictor of poor outcome. Stringent and timely epidemiological measures are crucial to curb the rapid spread. Ongoing efforts are needed to explore for an effective therapy (i.e., protease inhibitors, remdesivir, β interferon) for this emerging acute respiratory infection.
综上所述,2019-nCoV导致疫情迅速传播,人际传播,潜伏期中位数为3天,致死率相对较低。相当比例的患者在最初表现时没有发热和放射学异常,腹泻则不常见。疾病严重程度是不良预后的独立预测因子。严格和及时的流行病学措施对控制迅速蔓延至关重要。需要不断的努力来探索一种有效的治疗方法。、蛋白酶抑制剂、remdesivir β干扰素)这一新兴急性呼吸道感染。
7. Acknowledgment
7、感谢
We thank the hospital staff (see Supplementary Appendix for a full list of the staff) for their efforts in recruiting patients. We are indebted to the coordination of Drs. Zong-jiu Zhang, Ya-hui Jiao, Bin Du, Xin-qiang Gao and Tao Wei (National Health Commission), Yu-fei Duan and Zhi-ling Zhao (Health Commission of Guangdong Province), Yi-min Li, Zi-jing Liang, Nuo-fu Zhang, Shi-yue Li, Qing-hui Huang, Wen-xi Huang and Ming Li (Guangzhou Institute of Respiratory Health) which greatly facilitate the collection of patient's data. Special thanks are given to the statistical team members Prof. Zheng Chen, Drs. Dong Han, Li Li, Zheng Chen, Zhi-ying Zhan, Jin-jian Chen, Li-jun Xu, Xiao-han Xu (State Key Laboratory of Organ Failure Research, Department of Biostatistics, Guangdong Provincial Key Laboratory of Tropical Disease Research, School of Public Health, Southern Medical University)。 We also thank Li-qiang Wang, Wei-peng Cai, Zi-sheng Chen, Chang-xing Ou, Xiao-min Peng, Si-ni Cui, Yuan Wang, Mou Zeng, Xin Hao, Qi-hua He, Jing-pei Li, Xu-kai Li, Wei Wang, Li-min Ou, Ya-lei Zhang, Jing-wei Liu, Xin-guo Xiong, Wei-juna Shi, San-mei Yu, Run-dong Qin, Si-yang Yao, Bo-meng Zhang, Xiao-hong Xie, Zhan-hong Xie, Wan-di Wang, Xiao-xian Zhang, Hui-yin Xu, Zi-qing Zhou, Ying Jiang, Ni Liu, Jing-jing Yuan, Zheng Zhu, Jie-xia Zhang, Hong-hao Li, Wei-hua Huang, Lu-lin Wang, Jie-ying Li, Li-fen Gao,Jia-bo Gao, Cai-chen Li, Xue-wei Chen, Jia-bo Gao, Ming-shan Xue, Shou-xie Huang, Jia-man Tang, Wei-li Gu, Jin-lin Wang (Guangzhou Institute of Respiratory Health) for their dedication to data entry and verification.
我们感谢医院工作人员(完整的工作人员名单见附录)为招募病人所做的努力。我们感谢Drs的协调。Zong-jiu张Ya-hui娇,本·杜,Xin-qiang高和魏道(国家健康委员会),岳飞段和Zhi-ling赵(广东省卫生委员会),李Yi-min Zi-jing Liang Nuo-fu张Shi-yue Li Qing-hui黄黄洗脸和李明(广州呼吸卫生研究所)大大促进病人的数据的集合。特别感谢统计小组成员郑晨教授。(南方医科大学公共卫生学院广东省热带病研究重点实验室生物统计学系器官衰竭研究国家重点实验室)Wei-peng Cai,我们还要感谢李强Wang Zi-sheng Chen Chang-xing Ou, Xiao-min Peng Si-ni崔,元王,谅解备忘录曾庆红,鑫,Qi-hua他Jing-pei Li Xu-kai Li Wei,李敏欧,亚雷,经纬Liu Xin-guo Xiong, Wei-juna Shi, San-mei Yu Run-dong秦,羊绒衫姚明,Bo-meng张萧红谢,谢Zhan-hong Wan-di Wang Xiao-xian张Hui-yin Xu Zi-qing周,应江,倪,晶晶元,郑朱、张Jie-xia,洪涛,魏华黄Lu-lin王李洁英,高丽芬,高嘉波,李彩晨,陈学伟,高嘉波,薛明山,黄寿燮,唐家文,古伟立,王金林(广州呼吸健康研究所),他们致力于数据录入和验证。
点击下载英文原文:Clinical characteristics of 2019 novel coronavirus infection in China





